AirCARE1 recently provided a case study of a neonatal ECMO patient transport to the International Travel & Health Insurance Journal (ITIJ), featured in the Air Ambulance Review March Issue. Here is what the article said:
A neonatal patient on ECMO needed a short transfer within the US, which required very meticulous planning and preparation by AirCARE1’s air medical team
Case background
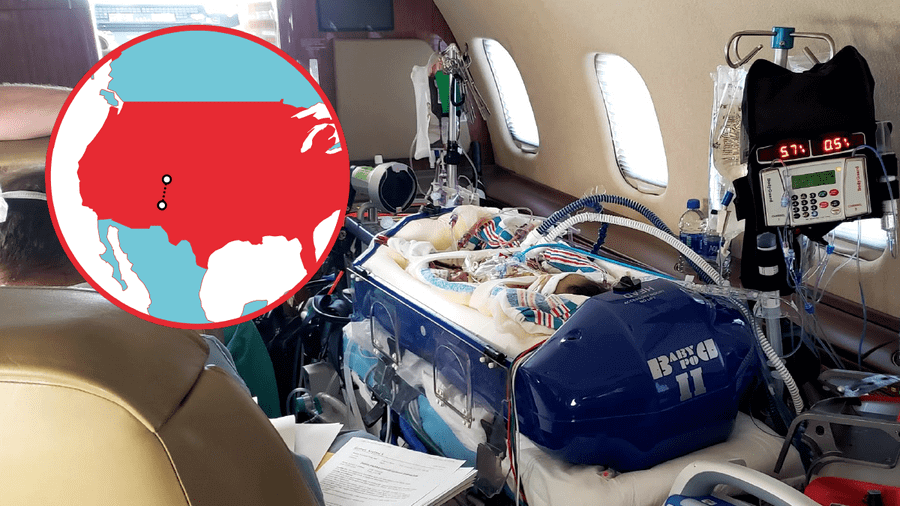
AirCARE1 was called to transport a seven-month-old infant who was currently on extra corporal membrane oxygenation (ECMO). This patient had been born prematurely and had been diagnosed with a chromosomal and cardiac abnormalities. The patient had a prolonged hospital stay due to several surgeries and was ultimately discharged from the hospital in March.
The patient had been doing fairly well at home until June, when they were admitted back to the hospital for low oxygen saturations and tachypnea. The patient was to undergo surgery to close a VSD and have a PA band takedown performed. Four days post-op, the patient had to be centrally cannulated for VA ECMO. This patient now required an air ambulance transport to a higher level of care which was a one-hour flight time away.
Risk mitigation
ECMO support is a highly specialized treatment modality that has inherent risks during transport, as there are many unique considerations needed for a successful flight. The first consideration was risk. Utilising our operational risk management tool, and the fact the patient was on ECMO, ventilated and on multiple drips, caused this flight to fall into a high-risk category that was mitigatable by placing an additional medical crew member on the flight roster. The team consisted of two cardiac perfusion specialists, one critical care flight nurse and two critical care flight paramedics, all of whom were trained in ECMO transports.
Complexities of the flight
Successfully transporting a critically ill patient requiring ECMO is a complex endeavour in and of itself. The complexity increased due to the young age and fragility of this patient, who weighed only 4.8 kilogrammes. For a child this young, there was simply no room for error, as any movement of just a few millimeters in the wrong direction of either the patient or cardiac circuit could dislodge the chest cannula, causing the patient to exsanguinate and die. Other complexities included managing multiple drips and ventilation of the patient while ensuring the patient did not inadvertently become extubated.
Flight considerations
Each ECMO trip is different and has its own unique set of challenges. Since this was an air ambulance transport, specific attention needed to be given to the flight environment’s effect on the patient. The flight environment leads to unique considerations with respect to atmospheric pressure, oxygenation, temperature, noise and vibration, and g-forces during acceleration and deceleration. More seriously, gas expansion can lead to life-threatening adverse effects on the patient if air bubbles are missed. Extreme care needed to be taken when switching the ECMO circuit over to the transport ECMO team’s circuit to ensure there was not even the smallest micro air bubbles in the system, which, if left unnoticed, could flow to various parts of the body, and cause major damage.
Upon arrival at bedside, the ECMO team had an extensive conversation with the mother and father regarding the numerous risks and potential complications of transporting such a critically ill patient. Due to the size of the ECMO team, neither mother nor father could accompany their child during flight. Both gave informed consent for this patient.
ECMO patient preparation for flight
The medical crew proceeded to enter the patient’s room and assess the patient. The patient was on multiple drips that included cardiac medications, paralytics, and anticoagulants. Additionally, the patient was on a ventilator with an uncuffed ETT and had four chest tubes, along with being on ECMO.
Each ECMO transport team has a team lead to ensure the preparation process is meticulously adhered to in order to prevent any inadvertent mishaps. Movement and conversation is highly controlled in order to maintain focus on the tasks at hand. In this particular instance, the patient’s IVs were moved over to the medical crews’ pumps first. After ensuring all drips were functioning properly, the patient was then transferred to the AirCARE1 Hamilton T1 ventilator and monitor. The patient was reassessed after each step to ensure they were tolerating each action. Transferring the patient to AirCARE1’s equipment first, and then transferring the patient to the ECMO circuit, was imperative to ensure any problems with the patient could be easily identified and attributed to either the equipment being utilised, or to the cardiac circuit.
While the team was preparing the patient for transport, the cardiovascular perfusionists were preparing the cardiac circuit. Since the patient was not on the same ECMO machine as the ECMO transport teams’ machine, the cardiac circuit had to be built and adapted correctly to ensure a smooth transfer. This included priming the circuit with platelets, red blood cells and FFP. Extreme care was taken during the switch to the air medical team’s ECMO machine. Multiple eyes were on the circuit to identify any possible air bubbles. Additionally, if the ECMO machine sensed any air, the machine would shutdown, leading to grave consequences for the patient.
Movement of patient
Finally, when everything was deemed ready, the current ECMO circuit on the patient was clamped with sterile clamps and the new circuit with its adapter was attached. After the final team stop to ensure everything was properly functioning, the patient was transferred to the baby pod on to the stretcher.
Transferring this patient to the stretcher took a high level of co-ordination to ensure the patient wasn’t moved in such a way that decannulated or extubated the patient. A person was assigned to watch the cannulation site, as well as the ETT, during transport to allow for safe movement. The packaging process took over four hours to complete as the crew had to be very methodical, precise, and meticulous.
Great care needed to be taken to ensure a smooth transport via the ground ambulance to and from the facilities, as well as loading the patient into the aircraft. Since the patient was ventilated and had a small uncuffed ETT, a medical crewmember was assigned to ensure the patient would not become extubated.
During the course of the transport, the patient was continuously monitored. The patient was transported to their destination which was only an hour of flight time away! The total mission time for this patient took eight and a half hours. The patient successfully tolerated the flight.
What we know
Successful ECMO flights take a highly trained and well-organised team who have a methodical approach to packaging the patient for transport. It is imperative the team work together and communicate effectively during the transport to ensure a safe and positive outcome for the patient.
Original Article Can Be Found At:
https://www.itij.com/latest/long-read/case-study-neonatal-ecmo-transport-within-us



{kind=link}
{kind=link}
{kind=link}